Behavioral economics
December 7, 2015
Why do some people choose not to take actions that they know would protect or improve their health?
Behavioral economics research provides one of the answers – people tend to focus upon immediate costs and benefits of taking certain actions, rather than on long-term benefits. Research increasingly has shown that relatively small rewards can spur action.

Drs. Harsha Thirumurthy (left) and Audrey Pettifor (Photo by Linda Kastleman)
Two UNC Gillings School of Global Public Health researchers are among those using behavioral economics to investigate whether people in sub-Saharan Africa will adopt behaviors that prevent the acquisition or transmission of HIV.
Harsha Thirumurthy, PhD, associate professor of health policy and management, conducted two studies to assess the effect of providing different types of low- cost incentives to Kenyan men who undergo medical male circumcision, a biomedical intervention proven to reduce the men’s risk of HIV acquisition. Audrey Pettifor, PhD, associate professor of epidemiology, conducted a six-year study examining the effect of cash transfers, conditional upon high school attendance, on young South African women’s risk of HIV acquisition.
There are differences, Thirumurthy explains, between targeted use of small financial and non-financial incentives and cash transfer programs that might seek, for example, to reduce overall poverty in a population. Incentives that seek to promote specific health behaviors can work across socio-economic levels because they reward immediate action – countering the tendency in all of us to delay certain health behaviors, even when we know they can be good for long-term health.
In one study in Kenya, Thirumurthy’s team tested different types of incentives by randomizing uncircumcised men into three groups – control, lottery incentives and fixed amount of compensation. The control group was offered a small amount of compensation (about $0.60) if they elected circumcision within a three- month time frame. The lottery incentives group could have a chance to win prizes, ranging in value from a $2.50 food voucher to a bicycle or smartphone, if they chose to be circumcised. The fixed compensation group was offered a food voucher equivalent to approximately $12.50 if they chose to have the procedure. The study results were striking.
“Only 1.3 percent of those in the control group underwent circumcision within the short three-month follow-up period,” Thirumurthy says. “In contrast, 8.4 percent of those who received fixed compensation underwent the procedure – more than six times as many – as a result of providing a small economic incentive. The fixed compensation helped offset the immediate cost of missing work while undergoing and recovering from the procedure, especially for men in manual labor jobs. It also helped counter the tendency to delay scheduling the circumcision.
Thirumurthy found that lottery-based incentives, commonly used in the U.S., were not as effective as the provision of fixed compensation. Only 3.3 percent of men in that group underwent circumcision.
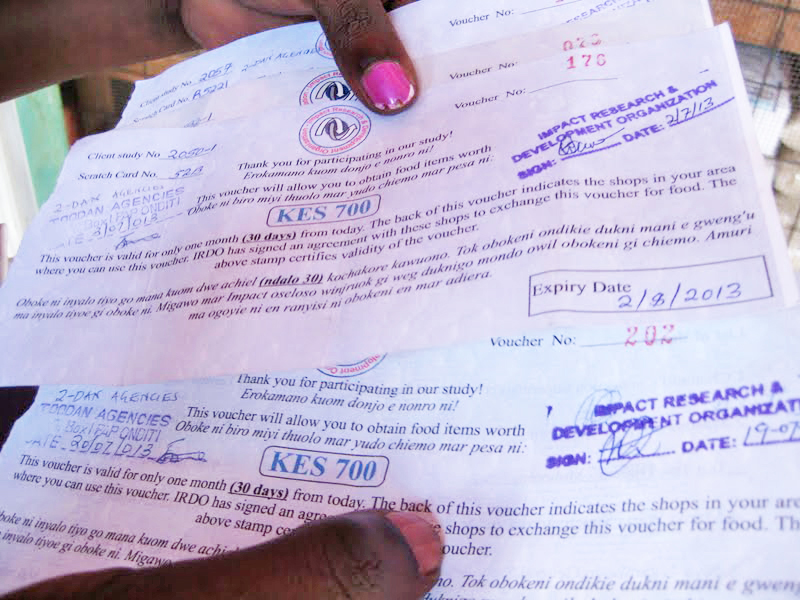
Dr. Harsha Thirumurthy found that food vouchers (above) could be an incentive for men in Kenya to undergo circumcision, a procedure that reduces risk of acquiring HIV. (Contributed photo)
Thirumurthy’s findings appeared in the November 2015 issue of the Journal of Acquired Immune Deficiency Syndromes. He led an earlier study, published in August 2014 in the Journal of the American Medical Association, which confirmed the power of small economic interventions (between $8.75 and $15 in food vouchers) to achieve higher levels of circumcision uptake.
In South Africa’s rural Mpumalanga Province, Pettifor has led the first randomized controlled trial to examine the impact of conditional cash transfers, related to high school attendance, on reducing HIV acquisition in young women.
Young women in sub-Saharan Africa are at incredibly high risk of HIV infection – 5 percent of South African girls have acquired HIV at age 15, and the infection rate climbs to 25 percent by the time the young women are in their early 20s. Ensuring that the girls attend high school regularly – and graduate – is one intervention that consistently reduces risk of HIV infection. However, financial and other barriers prevent many young women from completing high school.
“They can’t afford school fees, school uniforms, and transportation costs,” says Pettifor. “They may be responsible for caring for family members. Many household duties fall to them, so girls may be required to stay home while boys attend school.”
Schooling is thought to reduce HIV risk for several reasons. Girls who stay in school likely have greater exposure to HIV-prevention messaging and may have greater self-efficacy to act on prevention messages. They are more likely to have social and sexual networks of people who are lower risk, including friends and sexual partners who are closer in age. Pettifor and colleagues also hypothesized that providing money to young women and their families would reduce dependence upon male partners and reliance upon transactional sex to obtain money or goods.
A total of 2,533 young women, ages 13-20, were randomized into either a study group receiving cash transfers conditional on 80 percent school attendance or a control group receiving no cash transfers. Those in the study group received about $10 per month, and their families received about $20 per month. The amounts were selected because they are similar to the South African government’s Child Support Grant, which provides about $33 per month per child to poor South African families. If the intervention worked, says Pettifor, researchers could make a case for the government to carry on with it – a critical step for sustainability.
The results were surprising. Young women who received cash transfers reported reducing some risk behaviors, such as having unprotected sex or experiencing intimate partner violence, but Pettifor found no difference between the rate of HIV infection in the study and control groups. Perhaps most surprising, 95 percent of the girls in both groups remained in school.

These girls in South Africa’s Mpumalanga Province may be at decreased risk for acquiring HIV if they receive help to stay in school. (Contributed photo)
While the cash transfer did not change school attendance, it is likely that participation in the study increased attendance overall. School attendance among 17- and 18-year-olds not in the study was about 80 percent, closer to the national average. As Pettifor and colleagues had hypothesized, staying in school was protective for HIV infection. Young women who attended less than 80 percent of the time were three times more likely to acquire HIV during the study period.
Therefore, while the transfer was not needed in this study to encourage young women to attend school – likely because South Africa supports poor families in schooling their children – school was protective, and study findings reinforced the message to keep girls in school.
Pettifor and colleagues are conducting further analysis to determine whether particular subgroups benefited from the cash-transfer program and what other interventions might help prevent HIV acquisition.
A growing body of research suggests that small economic incentives can be useful for targeting specific health behaviors. For challenges such as the reduction of HIV risk among adolescent girls, more research may be needed to establish whether incentives to stay in school, in settings where school attendance is not high, can be effective in reducing HIV risk.
– Elizabeth Witherspoon
Thirumurthy and Pettifor credit their African study partners in collaborating to better understand ways that behavior-based economic incentives can move people to act in their own best interests, especially in the area of HIV/AIDS.
Thirumurthy’s Bill and Melinda Gates Foundation-funded research included colleagues Drs. Kawango Agot and Eunice Omanga, from Kenya’s Impact Research and Development Organization (tinyurl.com/irdo-kenya).
Pettifor’s study, HPTN 068, is part of the NIH-funded HIV Prevention Trials Network. Her partners included Dr. Kathleen Kahn, of the MRC/Wits Rural Public Health and Health Transitions Unit in the School of Public Health, and Dr. Catherine MacPhail, of the Wits Reproductive Health and HIV Institute (WRHI), both at the University of the Witwatersrand, in Johannesburg, South Africa.
A video about Pettifor’s work can be seen at tinyurl.com/pettifor-HIV-SouthAfrica.
Carolina Public Health is a publication of the University of North Carolina at Chapel Hill Gillings School of Global Public Health. To view previous issues, please visit sph.unc.edu/cph.