Beth Mayer-Davis
May 5, 2016
Eat better and move more — that’s the quintessential prescription for what chronically ails most people. It’s simple and effective, and it works for many.
However, for some, despite their wish to be healthier, the prescription isn’t enough. There may be too little money to buy nutritious foods. Parents working two jobs may believe they have too little time to exercise or may need more education about how to implement changes. Because genes also play a key role in the development of chronic diseases such as diabetes, diet and physical activity might not be enough to prevent illness. Attention to lifestyle is critical, however, in preventing many complications of this very serious disease.
These circumstances highlight the need for targeted interventions to promote healthy lifestyles in communities that face more than their share of chronic conditions.
Gillings School of Global Public Health researchers are involved in a number of efforts to prevent or better manage diabetes, from discovery to application. (See sph.unc.edu/global/diabetes.)
Elizabeth Mayer-Davis, PhD, the Cary C. Boshamer Distinguished Professor and chair of nutrition at the UNC Gillings School, is one of those who are known and respected globally. For 25 years, Mayer-Davis has led the charge against diabetes, combating it through nutrition.
“I’m engaged to improve population health,” said Mayer-Davis. “Social determinants are central to whether a person can succeed in preventing diabetes, can seek diabetes care if they’re diagnosed, and can care for themselves as they live with diabetes.”
Mayer-Davis has brought together academic, community and professional partners on several projects to fight diabetes.
.
Understanding the culture helps us face the challenge
Until the 1950s, there was no record of Type 2 diabetes in American Indian populations, but the disease began to surge in the 1960s and ’70s. Poverty, poor access to nutritious food, few opportunities and little support for physical exercise, and insufficient health education have added to the challenges.
“Reversing this trend among youth is critical, and the most effective strategy is weight management through healthful dietary choices and increased physical activity,” Mayer-Davis says.
However, effective interventions for weight management in American Indian youth have not been identified yet. In fact, even a “one-tribe-fits-all” approach won’t work, so Mayer-Davis’ team conducted a community-based participatory research study both with North Carolina’s Eastern Band Cherokee tribe and people from the Navajo tribe in Shiprock, Ariz.

Dr. Beth Mayer-Davis, at her standing desk, reviews the website for her Flexible Lifestyle Empowering Change (FL3X) project. (Photo by Linda Kastleman)
In a two-year, National Institutes of Health-funded study, the team enrolled 61 children and their parents in a multi-component intervention that included a 12-session after-school program. The program offered exercise for children and behavioral-change classes for parents and youth, supplemented by individual child and parent counseling to aid in motivation, goal setting and problem solving.
Mayer-Davis says a wide range of topics are discussed in the sessions, including how to select healthful foods (given local food availability and cost), how to cook and how to make physical activity fun.
“We tap into local culture in many ways, for example by incorporating native dance and native foods into classes,” Mayer-Davis says. “Native languages are used in all group sessions, and we celebrate local festivals, as appropriate. We provide opportunities for parents and their children to reflect on diet, physical activity and health and to develop specific goals and strategies to attain their goals.”
Understanding that families may face significant economic, medical or other difficulties, the program also provides resources and referrals when issues arise that are critical to the family’s overall well-being.
Initial results are promising. Children in the intervention have shown improvement in body mass index over time.
.
Diabetes and the American Indian community
The health-care challenges that American Indians confront run the gamut – from the Indian Health Service’s (IHS) being funded for healthcare costs at one-third per capita compared to the rest of the U.S. population, to the need for daily access to nutritious food (and, in some cases, safe drinking water), to the failure to address adequately the social determinants of health.
Individuals, health care practitioners, educational providers (including those who provide breakfasts and lunches and physical education), American Indian communities and national leaders all must take responsibility for understanding and incorporating social determinants into social, health and education programs and practices.
Research studies such as Dr. Mayer-Davis’ illustrate that there are interventions with promise to address the pandemic of diabetes. The challenge now is community sustainability of proven interventions. IHS and American Indian communities always will face difficulties meeting the sustainability challenge alone. The federal government administration and Congress also must live up to their responsibilities as were promised in treaties and established through Indian laws and policies.
—Charles Grim, DDS, MHSA, Deputy Executive Director, Cherokee National Health Services
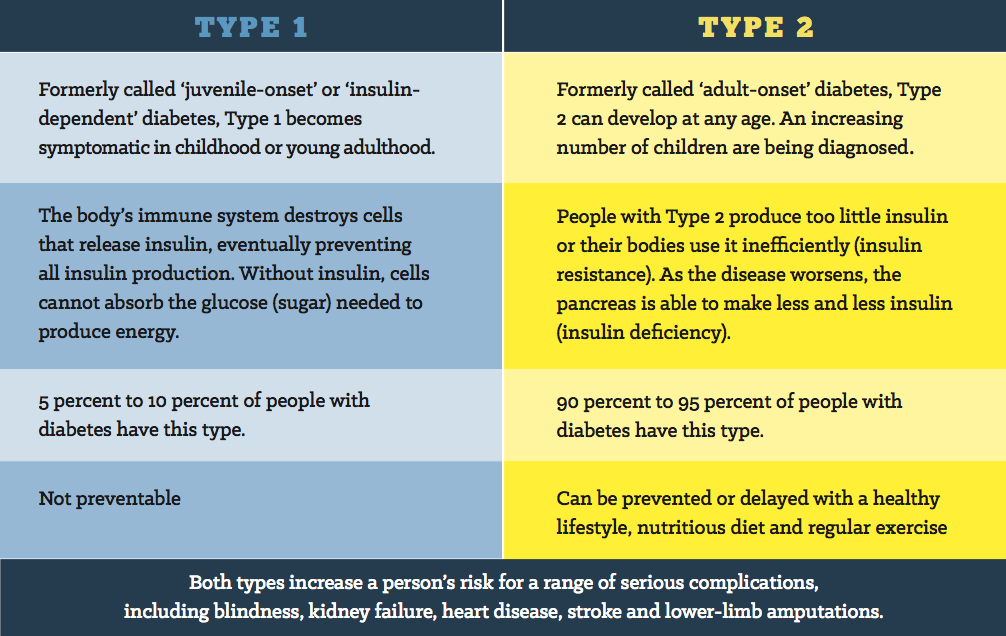
Type 1 diabetes
Traditionally, it was assumed that youth with Type 1 diabetes were invariably thin or of normal weight. Now, the prevalence of overweight and obesity in this group mimics the general population. Individuals with Type 1 diabetes face the same challenges related to weight management as anyone else, but also face unique challenges related to living with the disease.
Some youths choose not to take insulin to avoid gaining weight, thereby leaving their blood sugar uncontrolled. At the opposite end of the spectrum, low blood sugar requires treatment, typically with simple carbohydrates, and often is associated with hunger and overeating. Fear of low blood sugar can lead to avoidance of physical activity.
Mayer-Davis and colleagues have designed a behavioral intervention to help adolescents with Type 1 diabetes better control their blood sugar and maintain a healthy lifestyle. This intervention, called FL3X, is being tested in a multi-center randomized controlled trial funded by the NIH.
.
Chronic kidney disease
Chronic kidney disease (CKD) is a common and serious complication of diabetes.
“Nutrition is complicated for this group,” Mayer- Davis says. “CKD requires complex nutrition management designed to address kidney health, management of blood sugar and management of risk factors for cardiovascular disease.”
Through the Practice and Continuing Education (PACE) division in the nutrition department, which she established in 2015, Mayer-Davis collaborates with the Department of Medicine in the UNC School of Medicine. Renal dietitian and clinical assistant professor Shaun Riebl, PhD, RD, LDN, uses state-of-the-art behavioral strategies and motivational interviewing to help patients address their unique nutritional needs. The clinic also provides links to needed resources, including those addressing food insecurities.
“Dr. Mayer-Davis’ work at UNC Health Care is novel and provides smart and innovative ways to solve a population health challenge,” says Gillings School Dean Barbara K. Rimer. “By motivating patients with diabetes and helping them manage their individual nutrition needs, she empowers them to avoid rehospitalization.”
American Diabetes Association
Research-based knowledge is critical, but it is not effective unless translated successfully into clinical practice. Mayer-Davis’ close relationship with the American Diabetes Association, as board member and past president for health care and education, makes that transition easier.
She helped draft clinical guidelines and practice recommendations (see Diabetes Care, January 2014) and led a clinical trial on weight management strategies in rural areas. The trial demonstrated the importance of providing insurance reimbursement for a sufficient number of intervention hours if desired outcomes were to be achieved.
“Our study, ‘Pounds Off With Empowerment,’ highlighted the reality that you may have an effective intervention, but if you can’t pay for it, it will sit on the shelf,” she says.
Overall, her diabetes research has focused upon providing the best possible evidence-based care to solve problems related to diabetes and its complications.
“These experiences inspire my work in population health,” Mayer-Davis says. “We must determine how to integrate clinical care with community and public health services if we are to address the social determinants of health that may have a detrimental impact upon care.”
This is particularly critical for vulnerable populations, including youth and individuals living in under-resourced environments.
“Until the worlds of clinical care and community services meet,” Mayer-Davis says, “we’ll fall short of what we can do to support, care for, and optimize health and well-being for people living with diabetes and other chronic conditions.”
—Whitney L.J. Howell
Carolina Public Health is a publication of the University of North Carolina at Chapel Hill Gillings School of Global Public Health. To view previous issues, please visit sph.unc.edu/cph.